INTRODUCTION
The angiomyolipoma (AML) is a benign tumor of mesenchymal origin, compound by mature adipose tissue, aberrant blood vessels and smooth muscle, with a prevalence of approximately 1-3% of all renal masses. With the advance in diagnostics, an increase in AML has been observed.
Approximately 80% are sporadic and associated with tuberous sclerosis syndrome (TSC) 2 gene mutation, while up to 20% are associated with TSC which are related to the TSC 1 gene and sporadically with lymphangioleiomyomatosis (LAM).1,2
Although generally it is considered as a benign neoplasm, they have been described as an extension rare cases renal vein and inferior vena cava, plus regional infiltration ganglia, and even colon.
CLINICAL CASE
A 22-year-old female patient who was presented to the hospital emergency for pain abdominal diffuse. As medical history revealed that the patient was followed up in nephrology by chronic kidney disease (CKD) stage I, caused through bilateral renal angiomyolipoma in disease tuberous sclerosis, affecting skin (angiofibroma), liver (hamartomas), brain (hypointense subependymal nodules with calcifications) and kidney, they were controlled by the urologist and neurologist, and depression treatment. No hypertensive, diabetic or dyslipidemia.
She described hours of evolution diffuse abdominal pain without apparent cause, no hematuria or urinary symptoms. No digestive disorders was observed.
On physical examination it revealed supraventricular tachycardia and soft abdomen with tenderness without location, slight signs of peritoneal irritation and palpation of cysts. Right renal fist percussion was positive.
After performing laboratory analysis, hemoglobin (Hb) was found to be 7.8 g/dl which indicated urgent blood transfusion.
Abdominopelvic CT
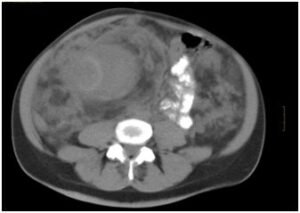
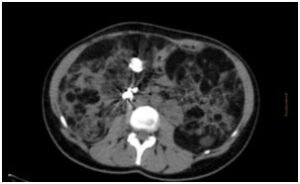
Patient with tuberous sclerosis and severe bilateral nephromegaly (>4 cm) will occupy more spec in the abdominal cavity leading to bilateral renal hamartomatous. A level mesograstrioempty right can be see none pseudo-capsular formation of approximately 10 cm major axis sonographically which corresponds to a clot. Inside it can be seen a right renal artery branch of aneurysmal size (2 cm). The vascularization of both kidneys is greatly increased (renal vein right 2 cm gauge) (Figures 1 and 2). Free fluid between intestinal loops and retroperitoneal due to bleeding from the right renal vasculature. Homogeneous splenomegaly about 15 cm major axis (Figure 3). With multiple spinal bones window blastic lesions are seen features of Bourneville disease.
Figure 1: TAC Abdominopelvic: free fluid between intestinal loops and retroperitoneal by bleeding from the right angiomyolipomas renal.
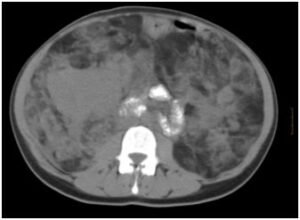
Figure 2: Increase of the abdominal perimeter

Figure 3: TAC Abdominopelvic: free fluid between intestinal loops and retroperitoneal by bleeding from the right angiomyolipomas renal.
The patient was evaluated by the urology department and underwent emergency surgery along with the vascular radiology with renal embolization via femoral Seldinger technique and percutaneously without complications (Figure 4).
Figure 4: Renal embolization.

She spent 4 years in treatment with low-dose sirolimus to try to decreasing size with good response angiomyolipoma clinic but from about 7 months ago she was accepted to start treatment everolimus 5 mg every 24 hours for inhibiting proliferation and the clonal expansion of antigen-activated T-cells (Figure 5). At present the patient is asymptomatic with impaired renal function but without worsening in recent reviews and she is awaiting further revisions to ensure effectiveness with decreasing size of angiomyolipoma.
Figure 5: TAC Abdominopelvic of control after the surgical and pharmacological treatment.
DISCUSSION
Angiomyolipomas renal tumors are uncommon, from the point of view histological consists of mesenchymal benign tissue, classified as hamartomas and variable portions composed of mature adipose tissue, fibers smooth muscle and blood vessels with irregular thickness devoid of elastic fibers.
In the last reviews one could have described also a percentage of evolution to malice of 34% to 65%, because of it of the importance of the follow-up.
The presentation of sporadic angiomyolipoma often is observed in women, with a 2:1 ratio (woman:men). The age of onset is 30 years, and most chances are unnoticed.
Approximately 20% to 30% of angiomyolipoma occur in patients with tuberous sclerosis and of these, up to 80% are bilateral.
Some authors postulate that renal angiomyolipoma, during pregnancy, may increase in size and increases the risk of spontaneous bleeding or retroperitoneal Wunderlich syndrome due to hormonal influence of this state.3
Diagnostic methods include ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), which has been a marked increase in the incidental diagnosis renal masses.
As discussed earlier, the association of renal angiomyolipoma is strongly associated with tuberous sclerosis, which is an autosomal dominant disease, with incomplete penetrance, so that approximately 50% of patients with this disease develop multiple hamartomas with involvement in brain, skin, retina, heart, lung and kidney.4
Tuberous sclerosis was recognized mainly by Friedrich von Daniel Recklinhausen in 1862, but the term was coined in 1880 Bourneville, so also it called Bourneville disease. Vougt described the classic triad of epilepsy, mental retardation and facial angiofibroma, but it just does occur 29% of cases, and 6% of patients with tuberous sclerosis cannot provide any of these findings.
Tumors larger than 4 cm associated with tuberous sclerosis are more susceptible to be symptomatic. Pain, hematuria and retroperitoneal bleeding are the most common manifestations, and if to the size the pregnancy adds, it becomes a diagnostic and therapeutic challenge.
Health care is still controversial in these patients. Oesterling and colleagues proposed as follow-up of the asymptomatic major tumors of 4 cm to realize echo or tomography every six months and in the minors of 4 cm of annual form. In symptomatic or bilateral tumors will be realized selective remobilization or conservative renal surgery (partial orlumpectomy).
Radical nephrectomy is carried out in case of uncontrolled bleeding or hemodynamic instability in large tumors, central location or coexistent carcinoma.5 Other treatment options include cryotherapy or tumor ablation heat either ultrasonic or radio frequency. Rapamycin is a derivative of the bacterium Streptomyces higruscopicus antibiotic, also known as sirolimus, important immunosuppressant used in organ transplants has shown benefit in years of study as well as the latest introduction to the treatment of everolimus, a drug from the same therapeutic group but a pharmacokinetic profile and greater oral bioavailability than sirolimus.
CONCLUSION
Renal angiomyolipoma is a disease of low prevalence, mostly incidental diagnosis, without requiring intervention more than I tracked by the urologist. However, when faced with patients with large tumor and/or multiple masses, coupled with clinical manifestations, there will be thinking among others, association with Lymphangioleiomyomatosis pulmonary and/or tuberous sclerosis, entities that constitute a challenge from diagnosis to treatment by a multidisciplinary group, in an attempt to improve the quality of life of affected. The managing focuses on the rapid diagnosis and the most effective treatment. The only management with periodic reviews is possible if the patient is stable or if it is the availability of embolization before surgery.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONSENT
The authors obtained written informed consent from the patient for submission of this manuscript for publication.





